고위험임신의 위험 요인과 미세먼지와의 연관성
Risk Factors of the High-Risk Pregnancy and Association with Particulate Matter
Article information
Trans Abstract
Purpose
High-risk pregnancy, resulting in major complications, such as abortion, gestational hypertension, and preterm labor, are on the rise, requiring intervention. Increased concentration of particulate matter that is 10 μ g per cubic meter or less in diameter (PM10) due to increased air pollution and industrialization has recently been noted as a risk factor for health problems, and prior studies have reported that PM10 is related to abortion, gestational hypertension, and preterm labor.
Methods
This study used data from the Korean medical panel between 2008 and 2016 to identify 879 women with normal pregnancies and 301 women diagnosed with high-risk pregnancies. The association between high-risk pregnancy and PM10 was analyzed using the annual average regional concentration du-ring the same period by the Korea Environment Corporation.
Results
At 35 years of age or older, the risk of abortion (p<0.001; 95% confidence interval [CI], 1.43–2.71) and preterm labor increased (p<0.05; 95% CI, 0.33–0.90). Married pregnant women were at a high risk of preterm labor (p<0.05; 95% CI, 0.25–0.98), and the prevalence of gestational hypertension was high in the metropolitan area (p<0.05; 95% CI, 12.09–25.93). On comparing the average annual concentration of particulate matter according to the level of atmospheric ventilation of the Korea Environment Corporation using a cutoff of ≤50 μ g/m3, the probability of preterm labor was 2.2 times higher in groups exposed to particulate matter concentration of ≥50 μ g/m3 (p<0.01; 95% CI, 1.49–3.25).
Conclusion
PM10 was related to preterm labor, and the risk of preterm labor was high if the average annual concentration of PM10 in the individual's residential area exceeded 50 μ g/m3.
서 론
고위험임신으로 진료받은 환자 수는 매년 증가하여 모자보건의 사회적 문제로 중재가 필요하다(Shin, 2012). 국내의 초혼연령이 높아짐에 따라 평균 분만연령도 높아져 고위험임신의 위험이 증가하고 있으며, 그 외에 인종, 사회경제적 지위, 미세먼지 및 환경오염물질 노출 등의 환경적 요인들의 영향도 받는다(Lee, 2014; Mä nnistö et al., 2015; Shin, 2012). Misra 등(2003)이 제시한 전생에 복 합결정요인 통합모델(integrating a life span approach with a multiple determinants model)에 따르면 임신 결과는 임신이 시작되기 훨씬 이전의 여성의 건강에 미치는 요인들과 연결된다. 이 모델에서 임신 결과에 영향을 미치는 요인으로 임부의 유전적 요인, 물리 환경적 요인, 사회 환경 요인으로 구성된 근 결정 요인(distal determinants)과 이것에 대한 민감도가 높은 원 결정 요인(proximal deter-minants)이 있다(Misra et al., 2003).
기존 연구에 따르면 고위험임신 중 유산(abortion)은 태아가 생존 능력을 갖기 전에 임신이 종결되는 것으로(Women's Health Nursing Research Society, 2020), 임부의 건강상태, 지역의 환경위생 및 임부의 사회·경제적 여건에 의해 영향을 받는다고 보고되었다(Han, 2003). 임신성고혈압(gestational hypertension)은 태아의 선천성 질환과 사망률로 이어질 수 있는 주요한 문제로 임부의 연령과 산과적 요인, 대기오염의 노출, 인종 등에 영향을 받는 것으로 나타났다(Kintiraki et al., 2015; Nobles et al., 2019; Savitz et al., 2014; Sepidarkish et al., 2017; Shin, 2012). 조산(preterm labour)은 제태기간 37주 이전의 분만으로 100만명이 넘는 신생아가 매년 조산으로 인한 합병증으로 사망하는 주요한 문제로(Howson et al., 2012), 연령과 사회·경제적 수준, 화학물질의 노출 등에 영향을 받는 것으로 보고되었다(Ferguson et al., 2014; Huynh et al., 2018; Parker et al., 2005; Zaman et al., 2019).
고위험임신의 위험 요인은 다양하며, 최근 환경적인 요인으로 미세먼지의 노출이 유산, 임신성 고혈압, 조산에 영향을 미치는 것으로 나타났다(Dadvand et al., 2014; Grippo et al., 2018; Liu et al., 2017). 미세먼지(parti-culate matter)는 지름이 10 μ g 이하의 먼지로 산업화가 진행되면서 주요한 환경 문제로 주목되고 있다. 우리나라의 경우 대도시를 중심의 연구는 많이 축적되었으나, 대부분의 연구가 개인 노출 수준에 대한 고려가 이루어지지 못 하였고, 민감 집단과 취약계층에 대한 고려가 부족하다고 보고되었다(Bae, 2014). 임산부는 대기오염 노출에 취약하며 미세먼지의 노출은 고위험임신 중 특히 유산, 임신성고혈압, 조산에 주로 영향을 미쳤다(Dadvand et al., 2014; Grippo et al., 2018; Liu et al., 2017).
고위험임신은 태아와 임부 모두에게 합병증을 일으키는 주요한 문제이며 저출산 시대에 주요하게 다뤄져야 할 문제이다. 고위험임신의 위험 요인 중 미세먼지와 관련한 국내 연구는 주로 단일 질환만을 다루었고, 국가데이터를 활용한 연구는 부족한 실정이다.
따라서 이 연구는 한국보건사회연구원과 국민건강보험공단의 의료패널데이터에서 임부 데이터를 추출하여 분석하고, 한국환경공단의 미세먼지 자료와 연계하여 고위험임신과의 연관성을 파악하고자 하며 구체적인 목적은 다음과 같다.
첫째, 임부의 일반적 특성에 따른 고위험임신의 위험 요인을 파악한다.
둘째, 미세먼지와 고위험임신과의 연관성을 파악한다.
대상 및 방법
1. 연구 설계
이 연구는 2008년부터 2016년까지 한국의료패널데이터의 자료를 활용하여 고위험임신의 위험 요인들을 파악하고, 한국환경공단의 대기오염 자료를 활용하여 미세먼지와 고위험임신과 연관성을 살펴보는 연구로서, Misra 등(2003)이 제시한 전생에 복합결정요인 통합모델(Integra ting a life span approach with a multiple determinants model)에 근거하여, 임신 결과에 영향을 미치는 원 결정 요인들을 바탕으로 이 연구의 개념적 모형을 설정하였다(Fig. 1).
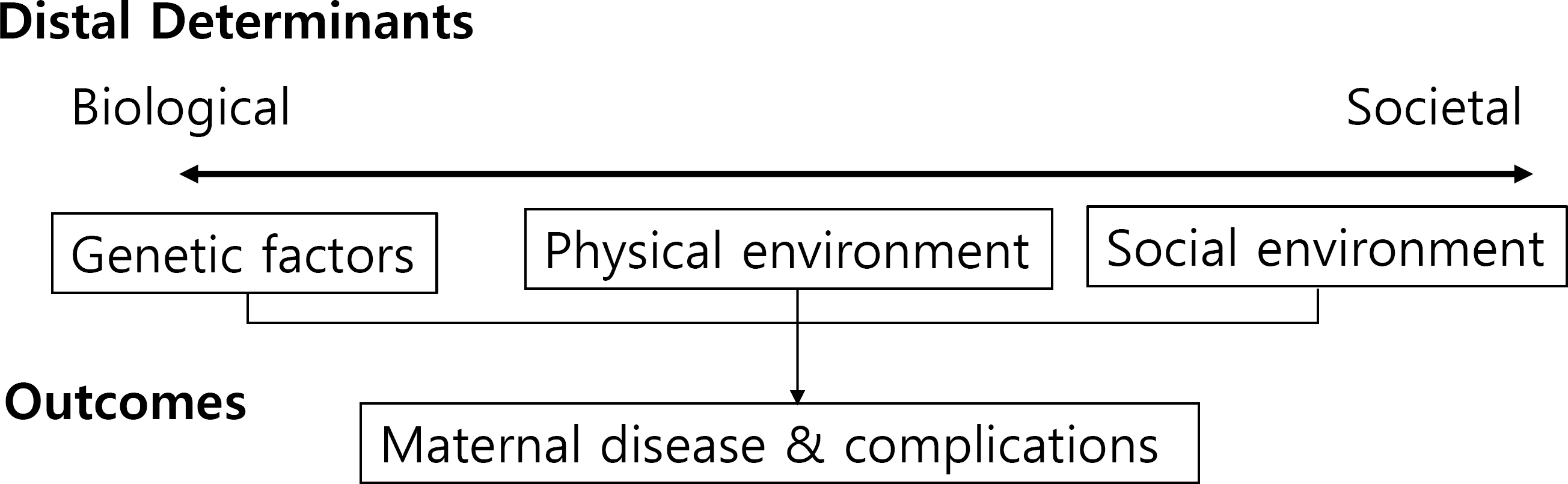
Conceptual framework of research.
2. 연구 자료
이 연구는 한국의료패널데이터와 한국환경공단의 대기오염 데이터 자료를 분석에 활용하였다. 미세먼지 자료는 한국환경공단에서 제공하는 도시별 대기 측정망 월별 평균 대기오염 농도 중 미세먼지(particles with a diameter of 10 μ m or less, PM10) 자료를 2008년부터 2016년까지 데이터를 연구 분석에 활용하였다. 2008년부터 2016년까지 의료패널데이터에 등록된 출산 경험이 있는 1,180명의 임부를 추출하여 정상 임부 879명, 고위험임부는 제7차 한국표준질병상인분류 개정에 따른 Korea Informative Classi-fication of Disease 분류로 유산(O03–06), 임신성고혈압(O13, O14.0–9, O15.0–9, O16), 조산(O60.0–3)을 진단받은 임부 301명의 데이터를 추출하여 연구 분석에 활용하였으며, 각 데이터당 등록되어 있는 대상자 거주지 정보를 바탕으로 한국환경공단의 미세먼지 농도 도시별 데이터와 비교하여 분석하였다.
3. 자료 분석
이 연구의 분석은 IBM SPSS Statistics ver. 25.0 (IBM Co., Armonk, NY, USA) 프로그램을 사용하여 고위험임신에 영향을 주는 위험 요인들을 파악하기 위해 t 검정(independent t-test)과 카이제곱검정(chi-square test)을 실시하였다. 임부의 일반적 특성에 따른 고위험임신의 위험요인들을 파악하기 위해 로지스틱회귀분석(logistic regression)을 실시하였으며, 미세먼지와 고위험임신과의 연관성을 파악하기 위해 카이제곱검정과 로지스틱회귀분을 실시하였다.
결 과
1. 연평균 미세먼지 농도와 고위험임신의 실태
의료패널데이터에 따른 연간 고위험임신의 발생은 2008년 전체 임부 233명 중 90명(38.8%)으로 가장 많았으며, 2015년 전체 임부 119명 중 18명(15.1%)으로 가장 낮았다. 2008년을 제외한 2009년부터 2016년까지 유산의 발생 비율이 가장 높았으며 다음 조산, 임신성고혈압이었다. 분석 결과는 Table 1과 같다.

Annual occurrence of high-risk pregnancy (n = 1,180)
한국환경공단의 자료에 따라 2008년부터 2016년까지 지역별 미세먼지(PM10)의 지역별 연평균 미세먼지 농도를 비교하였을 때, 주요 지역 대부분 2008년 연평균 농도가 높게 나타났으며, 지역별로 비교하였을 때 경기도가 다른 지역들에 비해 2008년부터 2016년 평균 농도 56.3 μ g/m3으로 가장 높게 나타났다. 고위험임신의 발생비율 또한 2008년이 29.9%, 경기 지역이 26.9%으로 가장 많았다. 분석 결과는 Tables 2, 3과 같다.

Annual average concentration (µg/m3) of PM10 by year and region

High risk pregnancy by year and individual's residence (n = 301)
2. 일반적 특성에 따른 고위험임신
대상자들의 일반적 특성 중 연령에 따라 유산(t=3.69, p<0.01)과 조산(t=−3.84, p<0.01)에서 차이가 있었다. 임부의 혼인상태에 따라 조산(χ2=5.79, p<0.05)에 영향을 주었으며, 임부의 거주지역은 임신성고혈압(χ2=11.66, p<0.01)에 영향을 주었다. 임부의 교육 수준과 직업은 고위험임신과 유의한 차이가 없었다. 분석 결과는 Table 4와 같다.
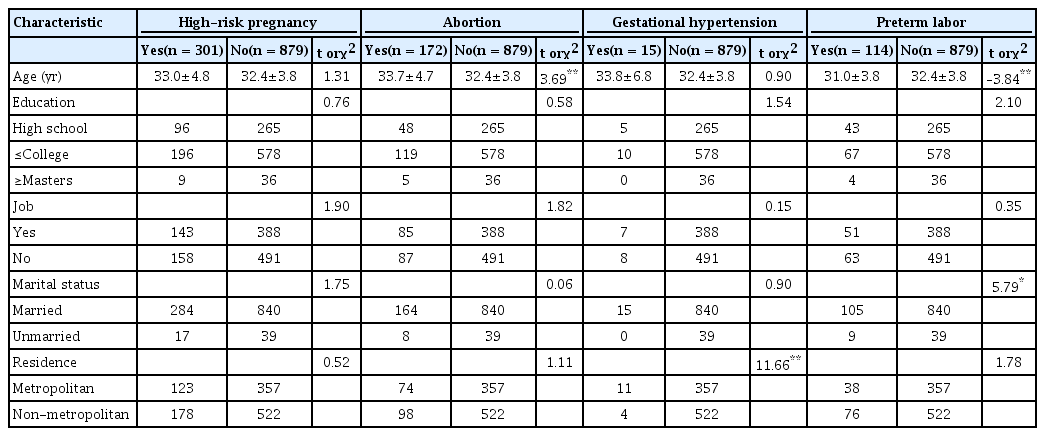
Risk factors of high-risk pregnancy by characteristics (n = 1,180)
3. 고위험임신의 위험 요인
연령이 35세 이상인 임부가 35세 미만인 임부에 비해 고위험임신이 발생할 비율이 1.31배 높았으며(p<0.05; 95% CI, 1.01–1.72) 유산이 발생할 비율이 1.97배 높았 으며(p<0.01; 95% CI, 1.43–2.71), 조산이 발생할 비율이 0.55배 높았다(p<0.05; 95% CI, 0.33–0.90). 기혼인 임부는 미혼인 임부에 비해 조산이 발생할 비율이 0.5배 높았으며(p<0.05; 95% CI, 0.25–0.98), 임부의 거주지역이 수도권인 임부가 비수도권인 임부에 비해 임신성고혈압이 발생할 비율이 7.37배 높았다(p<0.05; 95% CI, 12.09– 25.93). 임부의 교육 수준, 직업은 고위험임신에 영향을 미치지 않았다. 분석 결과는 Table 5와 같다.

High risk factors of high-risk pregnancy (n = 1,180)
4. 미세먼지와 고위험임신과의 연관성
거주지역에 따른 미세먼지(PM10)의 연평균 농도를 한국환경공단의 연평균 대기환경기준으로 50 μ g/m3 나누어 분석하였을 때, 임부의 거주지역의 미세먼지 연평균 농도가 50 μ g/m3 이하인 집단과 초과인 집단과의 조산 발생에 대해 차이가 있었으며(χ2=16.17, p<0.01), 거주지역의 미세먼지 연평균 농도가 50 μ g/m3 초과인 집단이 50 μ g/m3 이하인 집단에 비해 조산이 발생할 확률이 2.2배 높았다(p<0.01; 95% CI, 1.49–3.25). 분석 결과는 Tables 6, 7와 같다.

Association between high-risk pregnancy and annual average particulate matter

Association between high-risk pregnancy and annual average particulate matter
고 찰
이 연구는 고위험임신의 위험 요인을 규명하고 고위험임신과 미세먼지와의 연관성을 의료패널데이터와 한국환 경공단의 대기오염 자료를 통해 알아보고자 시도되었다.
임부의 연령은 유산과 조산과 관련이 있었으며, 사회적 요인인 임부의 혼인상태는 조산과 관련이 있었으며, 물리 환경적 요인인 임부의 거주지역은 임신성고혈압과 관련이 있었다. 이는 선행연구에서 35세 이상의 고연령 임부는 조산과 유산을 일으킬 수 있다고 하여(Jung, 2018; Lee, 2014), 이 연구의 결과를 지지하고 있다. 임부의 대표성을 위해 국내 모든 임부를 모두 추출한 국민건강보험 등의 국가 데이터를 사용한 고위험임신의 위험 요인에 대한 분석이 추가로 이뤄질 필요가 있다.
연평균 미세먼지 평균 농도와 고위험임신의 발생 비율을 보았을 때, 2008년 미세먼지 농도가 가장 높았으며, 고위험임신의 발생 비율도 가장 높았다. 지역별로 비교하였을 때에도 경기도 지역이 미세먼지 농도와 고위험임신의 발생 비율이 높았다. 이 연구 결과로 미세먼지는 조산과 관련이 있었으며, 거주지역의 미세먼지 연평균 농도가 50 μ g/ m3 초과인 집단이 50 μ g/m3 이하인 집단에 비해 조산이 발생할 확률이 2.2배 높았다. 선행연구에서 미세먼지(PM10)는 임신 전체기간동안 조산의 발생의 위험을 높이는 것으로 나타나, 선행연구는 이 연구의 결과를 지지하였다(Lamichhane et al., 2015). 이 연구는 다음과 같은 제한점이 있다.
이 연구의 대상자는 의료패널에서 제공한 데이터 중 임부만을 선택적으로 추출한 데이터로 일반적 성인과 다르게 임부가 가질 수 있는 여러 특성들이 제외되어 그에 따른 다양한 요인들을 분석할 수 없다는 제한점이 있으며, 이 연구의 결과를 모든 개인에 적용하기엔 제한이 있어 생태학적 오류(ecological fallacy)가 발생할 수 있다.
이 연구는 미세먼지 노출 농도를 넓은 범위인 도시별 노출 농도로 평가하였으며, 연단위의 평균 농도로 평가되어 더 세분화된 평가가 필요할 것으로 보인다. 선행연구들에 따르면 임신 전체 기간의 노출뿐만 아니라 분기별이나 주수별의 단기적 노출 영향 요인도 파악된 연구가 있으며, 대상자의 거주지를 기반으로 개인별 직접적 노출에 대한 평가도 필요할 것으로 보인다.
미세먼지는 대기의 온도와 기후 변화 등에도 영향을 받아 농도가 변할 수 있다. 고위험임신은 연령, 흡연, 음주 등 개개인의 특성에 따라 발생할 수 있다. 이 연구는 이를 통제하지 못했다는 제한점이 있으며, 통계적으로 연관성만 확인하여 추후 연구에서는 세부적인 변수들의 통제 아래 미세먼지와 고위험임신과의 생존 분석(survival analysis) 등의 여러 분석방법을 이용한 추가적 연구가 필요할 것으로 보인다.
결 론
이 연구 결과에서 임부의 연령이 35세 이상일 경우 유산과 조산의 위험을 높였으며, 기혼인 임부가 조산의 위험이 높았으며, 임부의 거주지역이 수도권일 경우 임신성고혈압의 위험이 높았다. 미세먼지는 조산과 관련이 있었으며, 임부의 거주지역 미세먼지 연평균 농도가 50 μ g/m3 초과할 경우 조산이 위험이 높았다.
이러한 연구 결과를 통해 미세먼지 노출에 취약계층인 임부에 대한 중재가 필요하며, 고위험임신의 위험 요인 파악과 미세먼지와의 연관성 연구에 대한 더 세부적인 데이터를 활용한 연구가 필요함을 밝힌다.
이해관계(Conflict of Interest)
저자들은 이 논문과 관련하여 이해관계의 충돌이 없음을 명시합니다.