서 론
또한, 2017년 우리나라의 초혼 연령은 남성이 32.9세, 여성은 30.2세로 남녀 모두 30세를 넘었다. 그리고 저체중아 구성비는 6.2%로 20년 전인 1997년에 비해 약 2배 증가했고, 조산아 구성비는 7.6%로 2007년에 비해 약 1.5배 증가했다(
Statistics Korea, 2018).
그리고, 보험연구원에 따르면, 난임자 수는 2006년 148,892명에서 2017년 기준 208,703명으로 연평균 3.1% 증가했으며, 난임자 중 남성의 비중은 2006년 15.5 %에서 2017년 29.9%로 늘어났다(
Kang & Kim, 2018).
국내 임신 출산 관련 통계들을 보면 향후에도 출산은 지속적으로 줄어들고 부정적 출산 결과의 악화가 예상된다. 이와 같은 국내 부정적 출산 환경의 개선을 위한 획기적인 정책 변화가 필요하고 임신을 원하는 가임기 남녀들을 위한 실질적 중재를 위한 사업의 필요성이 제기되고 있다.
미국 질병예방국은 “임신 전 관리” (preconception care)에 대해 예방 및 관리를 통해 여성의 건강 또는 임신 결과에 대한 생의학, 행동 및 사회적 위험을 식별하고 수정하는 것을 목표로 하는 일련의 중재로 정의하고 있다(
John et al., 2006).
한편, 남성도 임신 출산 관련하여 재생산의 한 축으로서 임신과 관련된 건강 행동의 주체로써 여성과 함께 임신 전 건강 관리를 하는 것이 중요하며 이는 흡연, 음주 및 운동과 같은 임신 건강 결정 요인에 대한 행동 변화에 중요한 영향을 미치는 것으로 알려져 있다(
Homish & Leonard, 2005,
2007).
이후 2013년 World Health Organization는 임신전건강관리의 중요성을 언급하고 있으며, 임신전 건강관리(Preconception care)는 임신 전 가임기 남녀에 대한 생의학적, 행동학적, 사회적 위험 요인을 파악하고 중재하는 예방적 차원의 관리로써, 산모와 태아의 건강증진을 목적으로 임신 전부터 남녀가 함께 건강한 임신과 출산을 도모하는 포괄적 관리를 의미한다고 하고 있다(
World Health Organization, 2013)
서울시는 2017년부터 서울시의 부정적 출산환경을 개선하기 위한 정책의 하나로 서울시 남녀 건강출산지원사업을 서울시, 서울시 자치구, 한국모자보건학회, 대한비뇨의학회를 비롯한 국내 난임전문가들과 진행해왔다. 이 사업은 2017년 서울시 4개지자체(중구, 성북구, 광진구, 양천구)에서 시작해서 2019년 12개 지차체로 확대된 후 2020년 서울시 25개 지자체로 확대되었다. 이 사업의 성과로 지난 2017년 11월부터 2019년 11월까지 참여 남녀들의 위험 요인 파악과 중재를 위한 프로토콜이 개발되어 적용되었으며, 해가 거듭하면서 개선되고 보완되었다. 총 참여 남녀 수는 9,546건이었다. 한편, 참여자들의 조사에서 참여자들의 100%는 이 사업이 필요하다고 답하였으며, 다음 임신준비 시에 재참여 의향은 97%, 그리고, 다른 가임 남녀에게 권장 의향은 98%로 나타났다(
Han, 2019).
저자들은 지난 3년 동안 이 사업을 통해 임신을 준비하는 남녀들에게 임신 준비에 필요한 설문과 검사를 통해 위험 요인을 파악하고 중재를 통해 실질적 도움을 주었고 만족도조사에서도 높은 만족도를 보였다.
그럼에도 불구하고 지난 3년 동안 여러 시행 착오를 겪었다. 예를 들면, 초기에는 위험 요인을 평가하기 위해 구글웹을 이용하여 설문을 진행했지만, 실제에 있어서는 서울시 지자체 컴퓨터에서는 구글 웹을 사용할 수 없어서 새롭게 웹을 개발하였다. 또 다른 예로는 난소기능을 평가하기 위한 항뮬러르관호르몬(anti-mullerian, AMH)검사 결과를 설명하는데 기준이 마련되지 않아서 혼란이 있었다. 이를 위해서 관련 전문가들이 모여서 검사 결과에 따른 안내지침을 마련하기도 하였다.
따라서, 이 사업의 시범사업을 통해서 얻은 성과들을 지속적으로 담보하고 새롭게 진입하는 서울시의 지자체뿐만 아니라 다른 지역의 지자체에서도 시행착오를 줄일 수 있도록 이 사업의 전반과 구성 내용들을 소개하고자 한다.
본 론
1. 사업 목적
서울시 남녀 건강출산지원사업은 임신을 원하고 있는 가임 남녀에게 임신에 장애가 되는 고위험 위험 요인을 조기 발굴하여 중재함으로써 임신 전부터 건강한 임신 준비에 역점을 둔 사업이다.
2. 사업 대상
가. 대상: 서울시 가임기 남녀
나. 신청 자격: 아래 대상임을 증빙(가족관계증명서, 주민등록증 등) 자료도 반드시 확인
1) 현재 서울시에 주민등록 또는 외국인 등록을 둔 서울시민
2) 부부 중 1명이라도 서울시에 주민등록 둔 시민이면 가능
단, 부부 모두가 외국인인 경우 각 국내체류자격 비자 (사증) 종류가 F-2 (거주), F-5 (영주), F-6 (결혼 이민)인 경우에 한함.
다. 신청 장소: 주민등록 주소지, 직장소재지에서 신청 가능
라. 신청 회수: 해당년 1회
3. 사업 내용
서울시 남녀 건강출산지원사업의 내용은 각 지자체의 보건소 담당자들에 의해 참여 남녀들의 설문 및 laboratory 검사를 통해 건강한 임신에 부정적 영향을 미치는 위험 요인들을 파악하고 정보 제공 및 상담 그리고 전문기관에 연계를 통해서 건강한 임신이 가능하도록 중재하는 것을 포함하고 있다(
Table 1).
T (tolerance: 주량으로 1회 음주량), W (worry: 음주에 따른 우려), E (eye-opener: 아침에 마시는 해장술), A (amnesia: 기억 잃음), K (cut down: 금주에 대한 생각)
전체 총 점수는 7점으로 T에서 1회 3잔 이상이라면 2점이고, 3잔 미만이라면 0점이다. 또한, W에서 금주를 권유받은 적 있다면 2점이다. 그리고 나머지 점수는 ‘예’인 경우 1점씩이다.
총 점수가 3점 이상이면 TWEAK 스크린 양성으로 유해한 음주(harmful drinking)군으로 평가되고 중재가 필요하다.
그리고, 불안 및 우울증 평가를 위해서는 수정된 Hospital Anxiety and Depression Scale을 활용한다. 홀수 쪽 항목은 불안증(anxiety), 짝수 쪽 항목은 우울증(depression) 평가를 한다.
8-10점은 경증의 불안 증상 또는 우울 증상이 있는 상태, 11-21점은 중등도 이상의 불안 증상 및 우울 증상이 있는 상태로 평가된다. 만약 점수가 8점 이상이면 스크린 양성으로 정신건강의학과에 연계를 통한 중재가 필요하다(
Table 3) (
Zigmond & Snaith, 1983).
검사(laboratory test)를 통한 참여 남녀에서 위험요인평가는
Table 4에서 보여주고 있다.
한편, 난임을 조기 스크린하기 위해서 여성의 경우 난소기능검사로 알려진 항뮬러르관호르몬(AMH)검사, 그리고 남성의 경우에는 정액검사(semen analysis)가 포함되어 있고 남성검진을 받을 수 있다. 남성검진은 대한비뇨의학회 회원 병원을 지정하여 참여 남성이 방문하여 정액검사 및 신체검진 후 결과 상담을 받을 수 있게 되어 있다(
Table 5).
나이 증가와 함께 AMH 수준이 감소한다. 주어진 나이에서 낮은 수준은 인공수정에 성공 가능성이 낮다. 한편, 높은 AMH 수준은 다낭소난소증후군의심, 난소과자극증후군(ovarian hyperstimulation syndrome)예측에 도움이 된다. 하지만, 이 검사만으로 난소 상태와 임신 능력을 평가하는 것은 한계가 있다. 임상에서는 난소기능을 평가하기 위해 초음파를 병행하고 있다(
Yoo et al., 2011).
AMH 검사에 대한 한계를 극복하고 검사 결과에 대한 올바른 안내를 위해서 난임전문가 및 보건전문가들이 참여한 자문위원회에서 안내를 위한 지침을 만들어 제공하였다(
Table 6).
설문 및 laboratory 검사에서 위험요인 발견 시 위험요인이 임신결과에 미치는 영향에 관하여 제공된 매뉴얼 내용을 참고하여 상담하고 중재가 필요한 경우
Table 7의 전문기관에 안내를 하고 있다.
4. 서울시 남녀 건강출산지원사업 참여 시 진행 과정
서울시 가임기 남녀들이 서울시 남녀 건강출산지원사업에 참여하는 과정은
Fig. 1과 같다. 위험 요인 평가를 위한 설문은 서울시의 웹사이트에서 지자체 보건소 방문 전에 완료한다. 보건소에 방문 시 laboratory 검사 처방은 지역보건의료정보시스템(Public Health Information System)을 통해서 행해지며, 검사 결과는 공공보건포털 G-health에서 확인 가능하며 검사 결과도 출력할 수 있다. 위험 요인 발견 시 각 지자체의 전담 보건요원에 의해 임신에 미치는 부정적 영향에 관한 정보 제공 및 중재가 필요한 경우 전문기관을 안내받는다.
5. 서울시 추진 경과 방향
서울시는 열악한 출산 환경을 개선하기 위해 남녀 건강출산지원사업을 2017년 7월부터 2018년 12월까지 한국모자보건학회와 함께 사업 모델을 개발하고 서울시 4개지자체(중구, 성북구, 광진구, 양천구)에 처음 적용하는 시범사업을 하였다. 2019년에는 12개지자체(중구, 성북구, 광진구, 양천구, 강남구, 동작구, 동대문구, 마포구, 성동구, 영등포구, 서대문구, 은평구)로 확대되었다. 그리고 2020년에는 서울시 25개 지자체 모두로 확대되었다. 또한, 시범사업을 시작하면서 건강한 임신준비 인식 개선 및 확산을 위한 홍보 활동을 강화를 위하여 웹툰, 카드뉴스, 매스미디어 등을 활용하였다. 또한, 이 사업의 내용과 폭을 넓히기 위해 건강한 임신과 출산을 위한 검사에 추가하여 난임을 조기에 스크린하고 치료하기 위해 여성의 경우 난소기능검사 AMH를 초기에 35세 이상 여성에 적용하는 것을 참여 여성 모두로 확대하였으며, 남성의 난임을 조기 발견하기 위해 남성건강검진으로 정액검사와 고환 등의 신체검진을 추가하였다. 또한, 이 사업의 초기부터 여성들의 독박임신, 독박육아를 해소하기 위해 임신에서 중요한 축인 남성이 적극적으로 참여할 수 있도록 하여 남녀가 함께 준비하고 참여하는 성인지적 환경강화를 위해 노력하였다(
Fig. 2).
6. 추진을 위한 각 기관별 역할
서울시와 지자체, 학계와 민간 전문기관이 협업하여 진행하고 있다. 또한, 학계의 모니터링단에 의해서 사업에 필요한 콘텐츠 제공과 업데이트를 통해 최상의 사업 프로토콜을 제공하고 있다. 또한, 사업내용과 과정에 대하여 각지자체에 방문 모니터를 통해서 사업의 표준화와 적정성을 평가하고 있다(
Fig. 3).
7. 사업성과 모니터링과 참여자의 만족도조사
사업성과 모니터링의 목적은 개발된 프로그램이 지자체에서 잘 구현되고 참여하는 남녀들이 불편함 없이 적용되는지를 평가하고 개선하기 위함이다. 또한, 이 사업에 참여하여 경험한 남녀들에게 본 프로그램을 타인에게도 추천할만한지, 이후에도 지속적으로 참여할 만한지 그리고 불편함에 관하여 평가하기 위하여 준비된 항목에 관하여 설문하였다.
1) 사업성과 모니터링
-시기: 정기적으로 상반기, 하반기 각 1회, 그리고 수시로 비정기적 모니터
-내용: 참여자의 사생활 보호가 가능한 사업의 공간/부서적정성, 사업인력의 교육 참여, 참여 인력의 지속성과 전문성, 사업진행 프로세스(이동 동선 및 서비스 내용), 상담 및 연계율, 지자체 인구 대비 참여율, 주말프로그램 운영 여부 평가함. 또한, 방문 시 지자체 담당자로부터 사업 진행과정에서 돌출되는 다양한 문제점 및 개선 필요 사항 등에 대한 전문적 자문
-방문 담당자: 모니터링 자문단(2인), 서울시 담당자(1 또는 2인)
2) 사업성과 만족도 조사
-조사 시기: 프로그램 참여 1개월 전후
-조사 방법: 리서치 전문기관을 통해 구조화된 설문을 통해 모바일 조사
-조사 내용: 본 프로그램 참여 자치구 보건소, 성별, 나이, 본 프로그램 사전인지, 이 사업이 얼마나 필요한지, 방문이 어렵지 않았는지, 프로그램담당자의 설명과 안내가 어렵지 않았는지, 친절하고 정중하였는지, 시간제약은 없었는지, 참여 후 건강한 아이 출산 자신감, 다음 임신 준비 시 참여 의향, 다른 가임 남녀에게 권장 의향에 관하여 물었다. 또한, 참여 남성 중 남성 건강검진에 참여자에게는 정액검사를 포함한 남성 건강검진이 얼마나 필요한지, 참여 시 병원 방문이 어렵지 않았는지, 병원 담당자의 설명과 안내는 어렵지 않았는지, 친절하고 정주하였는지, 시간 제약은 없었는지, 다른 가임 남성에게 권장 의향은 있는지를 물었다.
요약 및 결론
서울시 남녀 건강출산지원사업은 초저출산, 만혼, 저체중아 및 조산아율 증가로 출산 환경의 악화가 지속되는 국내 상황에서, 특히 서울시는 주거비용이 최근 급격히 증가하면서 주 출산연령인 30대의 거주가 더욱 어려워지면서 출산 환경을 획기적으로 개선하기 위한 정책이 필요한 상황에서 시작되었다. 이 사업은 서울시, 지자체, 그리고 학계가 협력하여 참여하는 남녀들에서 임신에 장애가 되는 위험 요인들을 파악할 수 있는 설문과 검사 프로토콜을 개발하고 2017년 7월부터 2018년까지 4개지자체에서 시범사업을 진행하였고, 2019년 12개지자체에서 시행하였다. 그리고 2020년 25개 지자체 모두로 확대되었다. 또한, 만혼에 따른 난임을 조기 발견하고 조기치료를 위해 여성의 경우 난소기능검사 AMH, 그리고 남성의 경우 정액검사를 포함하는 남성 건강검진을 시행하고 있다. 그리고, 이 사업에서는 여성들의 독박임신을 지양하기 위해 남성들의 프로그램 참여율을 높일 수 있도록 성인지적 환경 강화에 역점을 두고 있다. 또한, 이 사업의 문제점을 지속적으로 개선하고 업데이트하기 위해 서울시 담당자, 학계를 중심으로 한 모니터링단을 구성하여 지자체에 정기적으로 방문하고, 사업성과와 참여자들의 만족도를 조사하기 위하여 구조화된 설문을 통해 모바일 조사를 실시하고 있다.
향후, 이 서울시 남녀 건강출산지원사업이 초저출산 극복과 불량한 출산 환경을 획기적으로 개선할 수 있는 매우 의미 있고 중요한 사업이 되기 위해서는 보다 안정되고 확장성을 가질 수 있도록 서울시의 적극적인 관심과 지원, 이 사업의 결과로 확인될 수 있는 출산환경 개선관련 지표개발과 성과가 요구된다.
이해관계(CONFLICT OF INTEREST)
저자들은 이 논문과 관련하여 이해관계의 충돌이 없음을 명시합니다.
Fig. 1.
The process for participants of the preconception care. PA, posteroanterior; AMH, anti mullerian hormone.
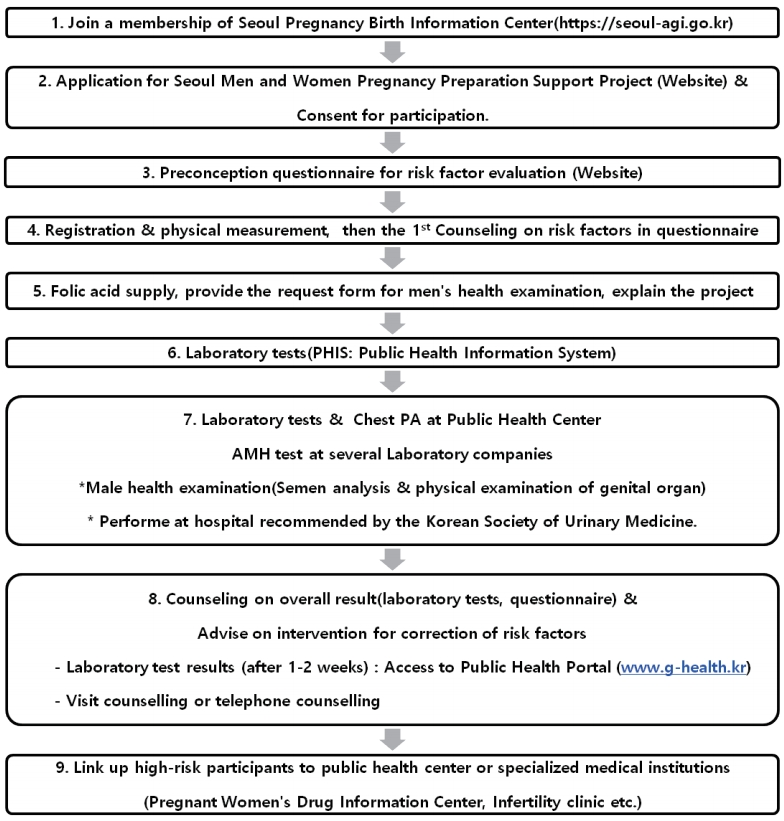
Fig. 2.
Vision progress and execution of the preconception care.

Fig. 3.
Role of participating agencies for the preconception care.
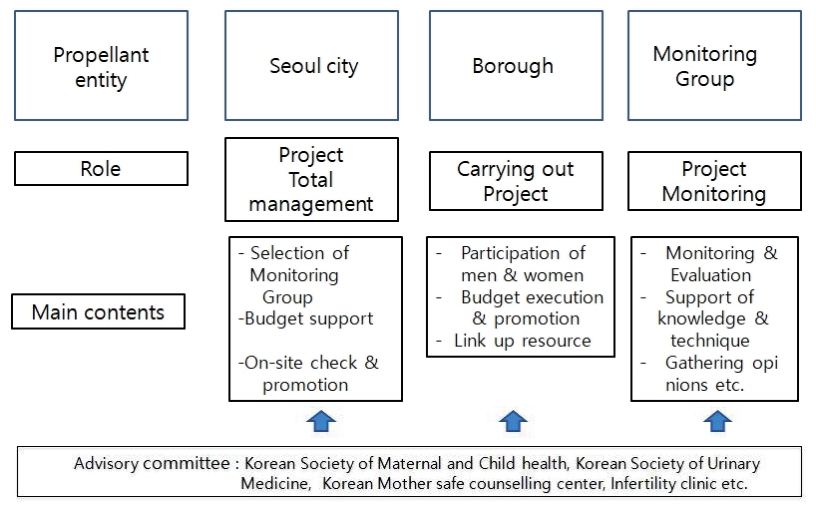
Table 1.
Contents for the preconception care
|
Component |
Details of the project |
|
Preconception questionnaire for risk factors |
1. Necessity: for evaluation and improvement of risk factors to promote healthy pregnancy before conception |
|
2. Target: men and women preparing for pregnancy |
|
3. Contents: lifestyle, environment, nutrition, medical history, infectious diseases and immunizations, drug use, family history, habitual drinking, mental illness, history of menstruation and pregnancy |
|
4. Method: online (Seoul Pregnancy and Birth Information Center) or off-line questionnaire |
|
Preconception laboratory tests for female |
1. Necessity: for detection and correction of immune susceptible women or abnormal findings on the laboratory test to promote healthy pregnancy before conception |
|
2. Target: childbearing women |
|
3. Contents: basic test -- CBC, LFT, TSH, ABO & RH, urine test, rubella immunity test, hepatitis B test, STD, and Chest PA; special test -- AMH |
|
4. Method: implementation of basic and special test by individual borough test results: Public Health Information System |
|
Preconception health screenings for male |
1. Necessity: for early detection and correction of male infertility or subfertility |
|
2. Target: male participants |
|
3. Contents: basic test -- CBC, LFT, TSH, ABO & RH, urine test, hepatitis B test, STD, Chest PA; special test -- physical examination for genital organ, semen analysis |
|
4. Method: implementation of basic and special test individual borough Test results: basic test - Public Health Information System; special test -- urology hospital |
|
Folic acid supply |
1. Necessity: prevention of congenital malformations |
|
2. Target: men and women preparing for pregnancy |
|
3. Content: taking folic acid before pregnancy |
|
Evaluation and counselling of risk factors |
1. Necessity: to provide an intervention program after evaluation of the risk factors associated with adverse pregnancy outcome |
|
2. Target: all participants |
|
3. Contents: evaluation and counselling of risk factors by questionnaire and laboratory test and physical examination of genital organ (only men) |
|
4. Method: counselling for preparing pregnancy of all participants and linkage to professional institutions such as Mothersafe Counseling Center, infertility clinic according to risk factors |
Table 2.
TWEAK Screening Test for the preconception care
|
TWEAK |
Questions |
Score |
|
T |
How many drinks does it take to make you feel high? |
□ Less than 3 cups (0 point) |
|
□ More than 3 cups (2 points) |
|
W |
Have close friends or relatives worried or complained about your drinking in the past year? |
□ No (0 point) |
|
□ Yes (2 points) |
|
E |
Do you sometimes take a drink in the morning when you first get up? |
□ No (0 point) |
|
□ Yes (1 point) |
|
A |
Has a friend or family member ever told you about things you said or did while you were drinking that you could not remember? |
□ No (0 point) |
|
□ Yes (1 point) |
|
K |
Do you sometimes feel the need to cut down on your drinking? |
□ No (0 point) |
|
□ Yes (1 point) |
Table 3.
Hospital Anxiety and Depression Scale (HADS) for the preconception care
Tick the box beside the reply that is closest to how you have been feeling in the past week. Don’t take too long over you replies: your immediate is best.
|
|
D |
A |
|
D |
A |
|
|
|
I feel tense or 'wound up': |
|
|
I feel as if I am slowed down: |
|
3 |
Most of the time |
3 |
|
Nearly all the time |
|
2 |
A lot of the time |
2 |
|
Very often |
|
1 |
From time to time, occasionally |
1 |
|
Sometimes |
|
0 |
Not at all |
0 |
|
Not at all |
|
|
I still enjoy the things I used to enjoy: |
|
|
I get a sort of frightened feeling like 'butterflies' in the stomach: |
|
0 |
|
Definitely as much |
|
0 |
Not at all |
|
1 |
|
Not quite so much |
|
1 |
Occasionally |
|
2 |
|
Only a little |
|
2 |
Quite Often |
|
3 |
|
Hardly at all |
|
3 |
Very Often |
|
|
I get a sort of frightened feeling as if something awful is about to happen: |
|
|
I have lost interest in my appearance: |
|
3 |
Very definitely and quite badly |
3 |
|
Definitely |
|
2 |
Yes, but not too badly |
2 |
|
I don't take as much care as I should |
|
1 |
A little, but it doesn't worry me |
1 |
|
I may not take quite as much care |
|
0 |
Not at all |
0 |
|
I take just as much care as ever |
|
|
I can laugh and see the funny side of things: |
|
|
I feel restless as I have to be on the move: |
|
0 |
|
As much as I always could |
|
3 |
Very much indeed |
|
1 |
|
Not quite so much now |
|
2 |
Quite a lot |
|
2 |
|
Definitely not so much now |
|
1 |
Not very much |
|
3 |
|
Not at all |
|
0 |
Not at all |
|
|
Worrying thoughts go through my mind: |
|
|
I look forward with enjoyment to things: |
|
3 |
A great deal of the time |
0 |
|
As much as I ever did |
|
2 |
A lot of the time |
1 |
|
Rather less than I used to |
|
1 |
From time to time, but not too often |
2 |
|
Definitely less than I used to |
|
0 |
Only occasionally |
3 |
|
Hardly at all |
|
|
I feel cheerful: |
|
|
I get sudden feelings of panic: |
|
3 |
|
Not at all |
|
3 |
Very often indeed |
|
2 |
|
Not often |
|
2 |
Quite often |
|
1 |
|
Sometimes |
|
1 |
Not very often |
|
0 |
|
Most of the time |
|
0 |
Not at all |
|
|
I can sit at ease and feel relaxed: |
|
|
I can enjoy a good book or radio or TV program: |
|
0 |
Definitely |
0 |
|
Often |
|
1 |
Usually |
1 |
|
Sometimes |
|
2 |
Not Often |
2 |
|
Not often |
|
3 |
Not at all |
3 |
|
Very seldom |
Table 4.
Laboratory test for the preconception care
|
Laboratory test |
Application for male or female |
|
Hemoglobin/hematocrit |
All |
|
Urine analysis: bacteria/WBC/RBC |
All |
|
Rubella IgG/IgM |
Female |
|
HBS Ag/Ab |
All |
|
Fasting blood sugar |
All |
|
SGOT/SGPT |
All |
|
BUN/creatinine |
All |
|
Syphilis |
All |
|
Human immunodeficiency virus |
All |
|
Thyroid stimulating hormone |
Female |
|
Anti-mullerian hormone |
Female |
|
Semen analysis |
Male |
|
Chest PA |
All |
Table 5.
Result of semen analysis and physical examination for men
|
◈ Reception number: ◈ Medical institution: ◈ Institution number: ◈ Medical doctor: ◈ Patient name: ◈ Birth date: ◈ Chart number: ◈ Inspection date: ◈ Report date: ◈ Marriage status: Marriage ◈ (Marriage date: ) Single □ |
1. Semen analysis results
|
|
Essential tests |
Results |
Reference value |
|
|
Semen volume (mL) |
|
1.5 or greater |
|
Sperm counts (106/mL) |
|
15 or greater |
|
Total motility (%) |
|
40 or greater |
|
Morphology (normal form) (*Strict morphology) (%) |
|
40 or greater (*4 or greater) |
|
pH |
|
7.2 or greater |
|
White blood cell (106/mL) |
|
< 1 (or 0-1) |
|
Red blood cell (106/mL) |
|
< 1 (or 0-1) |
|
Etc. |
|
|
|
|
2. Physical examination of genital organ |
|
◈ testis (volume, etc.) ① Normal □ ② Abnormal □ |
|
◈ scrotum(varicocele, etc.) ① Normal □ ② Abnormal □ |
|
◈ penis ① Normal □ ② Abnormal □ |
|
◈ Etc. (external meatus,etc.) ① Normal □ ② Abnormal □ |
|
|
3. Summary of examination results and counselling details |
|
① Normal □ |
|
② Abnormal □ Findings : ______________________________________ |
Table 6.
Recommendation according to anti-mullerian (AMH) levels
|
1. Regardless of the inspection agency, the AMH levels shall be based on the percentile according to the female age. |
|
2. If the AMH level is from less than 50 percentile to above 10 percentile, the ovarian reserve may be reduced. If she wants to get pregnant, she is considering to visit an infertility clinic. |
|
3. If the AMH level is less than 10 percentile, the ovarian reserve is definitely reduced. If she wants to get pregnant, she is strongly advised to visit an infertility clinic as soon as possible. |
|
4. Regardless of the AMH level, woman of greater than 38 years old, she is strongly recommended to visit an infertility clinic if she wants to get pregnant. |
|
5. If the AMH level exceeds 5 ng/mL and there are symptoms of polycystic ovarian syndrome (PCOS)*, she is recommended to visit an infertility clinic regardless of age. |
Table 7.
Referral clinic and institution for high risk group
|
Clinics or institutions |
Purpose for referral |
|
Mothersafe Counseling Center (1588-7309) |
Participants can get information about teratogenicity of their disease and exposure to medications, ethanol, cigarette smoking, etc. |
|
Department of Psychiatry (Public Health Center, Hospital) |
Participants who is screen positive in Hospital and Anxiety Depression Scale are referred to department of psychiatry. |
|
If the status of psychiatric disease is not controlled before conception and during pregnancy, their pregnancy outcomes are not favorable. |
|
Department of Internal Medicine (Public health center, hospital) |
Treatment of chronic disease including thyroid dysfunction, diabetes, high blood pressure, asthma, etc. |
|
Department of OB & Gyn (Public Health Center, Hospital) |
Evaluation and treatment for recurrent abortion, premature birth, congenital malformations in previous baby, history of mental retardation, etc. |
|
Metabolic Disorder Clinic (Public Health Center, Hospital) |
BMI 25 kg/m2 or higher (overweight, obesity) can cause adverse pregnancy outcome such as congenital malformations, gestational diabetes, and macrosomia etc. |
|
Smoking Clinics (Public Health Center, Hospital) |
Cigarette smoking can cause oral cleft, growth restriction, sudden infant death syndrome, ADHD, etc. |
|
Alcoholism Clinic (Public Health Center, Hospital) |
Screen positive of TWEAK test is associated with harmful alcohol exposure and habitual heavy alcoholism. Maternal alcohol exposure can cause fetal alcohol syndrome. |
|
Urinary Medicine Clinic |
Abnormal semen analysis or abnormal physical examination of genital organ (e.g., varicocele) can cause male infertility. |
|
Infertility Clinic |
Women over 38 years old, AMH abnormality |
|
If elderly women (35 years old or older) and have not been pregnant for 6 months without contraception. |
|
If women (less than 35 years old) and have not been pregnant for 1 year without contraception amenorrhea, menstrual irregularity, dysmenorrhea |
|
Vaccination (Public Health Center, Hospital) |
Vaccination of MMR, hepatitis B, HPV, varicella, Influenza, etc. |
REFERENCES
Almog B, Shehata F, Suissa S, Holzer H, Shalom-Paz E, La Marca A, et al. Age-related normograms of serum antimüllerian hormone levels in a population of infertile women: a multicenter study. Fertil Steril 2011;95:2359-63. 2363.e1


Chan AW, Pristach EA, Welte JW, Russell M. Use of the TWEAK test in screening for alcoholism/heavy drinking in three populations. Alcohol Clin Exp Res 1993;17:1188-92.
Han JY. The meeting for the final report and advisory council of Community-based Preconception care for male and female of childbearing age in Seoul Seoul (Korea), Seoul Metropolitan Government, 2019.
Homish GG, Leonard KE. Alcohol use and partner expectations among newly married couples. Subst Use Misuse 2007;42:1427-41.
John K, Posner SF, Biermann J, Cordero JF, Atrash HK, Parker CS, et al. Recommendations to improve preconception health and health care--United States. A report of the CDC/ATSDR Preconception Care Work Group and the Select Panel on Preconception Care. MMWR Recomm Rep 2006;55(RR-6):1-23.
Kang SH, Kim DG. The increase of infertility and subfertility in the times of low birth rate and the role of insurance [Internet]. Seoul (Korea), Korea Insurance Research Institute, 2018;Apr 2, [cited 2020 May 2]. Available from:
http://www.kiri.or.kr/report/downloadFile.do?docId=684
La Marca A, Sighinolfi G, Giulini S, Traglia M, Argento C, Sala C, et al. Normal serum concentrations of anti-Müllerian hormone in women with regular menstrual cycles. Reprod Biomed Online 2010;21:463-9.
World Health Organization. Meeting to develop a global consensus on preconception care to reduce maternal and childhood mortality and morbidity [Internet]. Geneva (Switzerland), World Health Organization, c2020;[posted 2013 Feb 5; cited 2020 May 2]: [67 p.]. Available from:
https://apps.who.int/iris/handle/10665/78067
Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand 1983;67:361-70.









